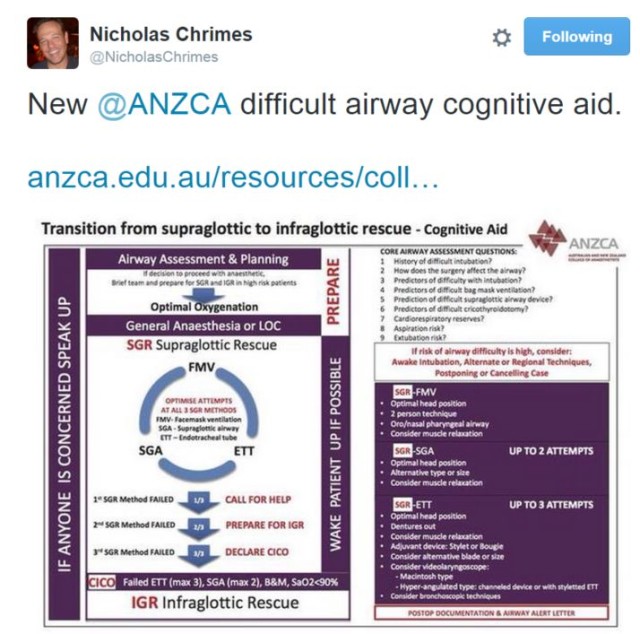
Thanks to the inimitable Dr Nicholas Crimes for this great resource. Very pleasing to see a good collection of algorithms in the appendices of the document, in the spirit that we have tried to create here.
A more thorough review to follow, but it is usually hard to fault our Antipodean friends.
Click the image to go to the article on Anesthesiology News
This month’s edition of Anesthesiology News features a worthwhile piece from Prof John Doyle, in which he poses 7 questions on the current state of airway management to 6 airway experts from around the world (Abdelmalak, Cooper, Frova, Rosenblatt, Spiegel and Doyle himself), and collates their responses into a dialogue. Definitely worth reading to determine what some (certainly not all) of the biggest names in the world are thinking on:
For what it is worth, here are my own answers, distilled into one-liners. I’m very willing to enter into discussions about them!
Place for DL in the future: Definitely; just look at the huge needs in the Third World and then ask if (even very cheap) VLs are a priority.
Use of bougies: Along with good positioning and mastery of face-mask skills, I think this is one of the most neglected parts of airway training.
What airway algorithm: The expert can do what they wish; the trainee should learn something appropriate (like ASA or DAS); the infrequent practitioner should use the Vortex.
Trache vs Cric: Cric all the way; scalpel-finger-bougie
Impact of VL in AFOI: Definitely reducing the use of AFOI, but a flexible scope remains an essential tool, and every airway master should be competent in it’s use.
Favourite SGA: Would love to say the 3gLM, but we need to publish the research first…
Favourite VL: Hasn’t been invented yet, but watch this space. The C-MAC with Pocket Monitor is my daily workhorse, but I have (and use) GlideScope, McGrath, AirTraq, King Vision, etc.
There are a lot of excellent (and complementary) views expressed in the article, which are worth reading. Check it out!
My friends over at #badEM are doing some sterling work to put Africa on the #FOAM map. This latest post, with some practical investigation by flight medic Jo Park-Ross deserves a good hard look and some introspection. She makes an impassioned plea for the use of cuff pressure manometers in the aeromedical environment (as they should be used wherever patients are intubated) with the practical demonstration of why it is so important. Please go and check it out on #badEM.
A recent explosion of Twitter discussion led me to do a quick search to refresh my own recollection on this topic – the number of intubations to become proficient (ie: what is the learning curve to reach X level of success?) My memory has a figure of 50-80 based on the level of expertise and setting, but it is always a good idea to refresh one’s grasp of the literature on the subject. I present here the results of a brief literature search – please note that I have not reviewed these papers more than a cursory inspection, so make your own conclusions. (To be updated if time allows). There is a little FOAM on the subject. While this is certainly not intended to be an exhaustive review or meta-analysis of the subject, here are various resources and studies to help answer this question:
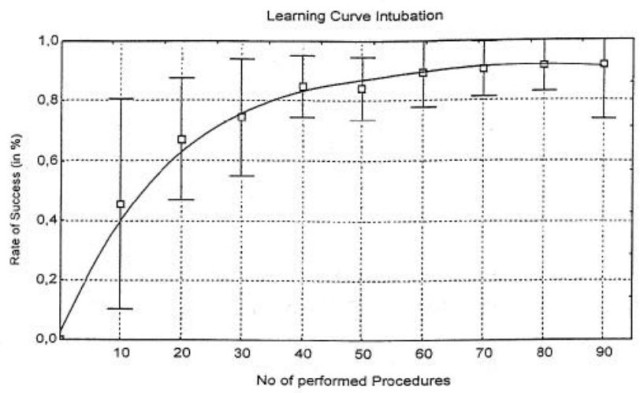
Konrad et al in Anesth Analg 1998: Found that intubation was the easiest of anaesthesia procedural skills to learn by anaesthesia residents amongst those studied (ETI>Spinal>Epidural>Brachial block>Arterial line), with 90% success rate being reached at a mean of 57 procedures. However, even after 80 intubations, 18% still required assistance. Check out the paper here.
Konrad 1988. Click image to access the paper.
De Oliveira Filho in Anesth Analg, 2002: 895 intubations by 7 anaesthesia residents used to create a cumulative sum success (CUSUM) model. 4/7 residents reached acceptable success (80%…!) after 79 +/- 47 endotracheal intubations (ETIs). Article here.
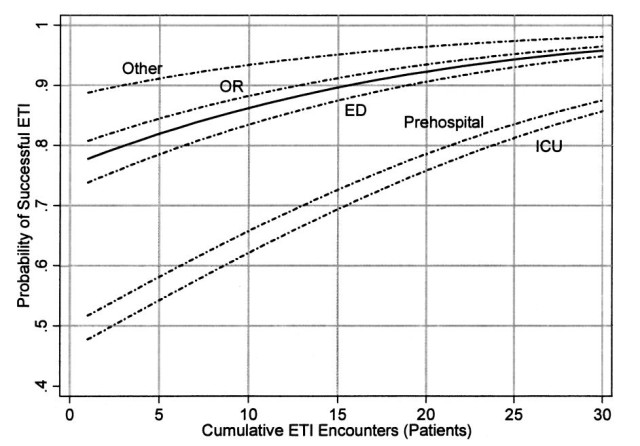
Wang et al. in PEC, 2005: Data from 60 US paramedic training programs over a two year period. Few students (4%) performed more than 30 ETI’s; almost none more than 50. Complex statistical model predicted 90% success rate (SR) after ~16 intubations, but there was significant difference depending on where these intubations took place (OR vs. ED vs ICU vs. preshospital), with the latter requiring significantly more practice, Paper online here.
Wang et al 2005 PEC. Click on the image to access the paper online.
Savoldelli et al in Eur J Anaesthesiol, 2009: The type of laryngoscope matters. In a mannequin, the learning curve flattened most rapidly with the AirTraq and Macintosh laryngoscopes, whereas the McGrath and Glidescope reached a later plateau with residual delay in speed of intubation. Paper not open access; see PubMed.
Komatsu et al in Anesthesiology, 2010: 9/15 non-anaesthesia interns showed a median requirement of 35 ETIs to achieve 80% success. Where a 90% SR was used, only 1/15 reached this level in 35 attempts. More interns were able to learn acceptable face-mask ventilation skills within a limited number of cases than ETI. See paper at Anesthesiology online here.
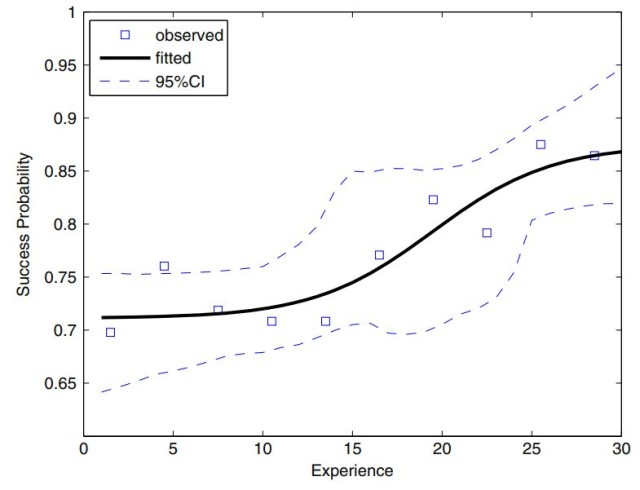
Toda et al in IJEM, 2013: 1045 ETIs by 32 paramedics in the OR. First-pass success rates over 30 attempts ranged 71-87%, but complications still averaged 31% after 30 attempts! 90% SR not achieved in 30 intubations by the majority of participants. Sinusoidal learning curve that showed little increase in success until after ~13 patients. Click here or the image to read the paper online.
Toda et al. Click on the image to access the paper online.
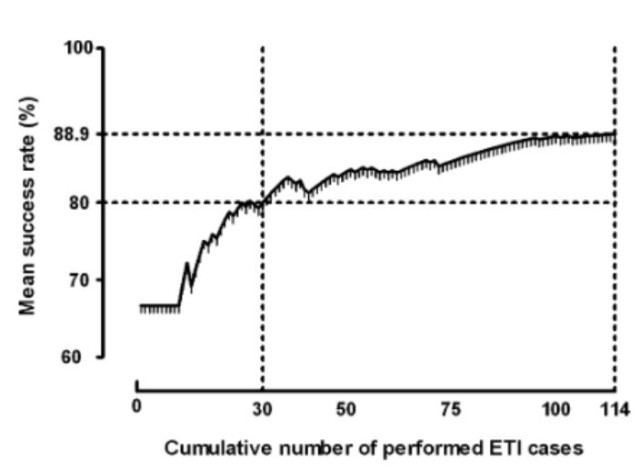
Je et al. in EMJ, 2013: Cumulative summation learning curve of 3 junior emergency medicine residents (first 2 years of EM training) looked at 90% proficiency (success rate [SR} of 90%), and found the mean number of endotracheal intuabtion (ETI) cases to achieve this was 75 (74.7; 95% CI 62.0 to 87.3). 80% SR was achieved after ~30 cases. Noteably, competency continued to improve after >100 cases. See here on ResearchGate to access the paper.
Je et al EMJ 2015 – click image to access the paper on ResearchGate
Rujirojindakul et al, in Anes Research Prac, 2014: Cumulative summation technique evaluating 11 nurse anaesthetists in the first 3 months of their training. SR of 80% deemed acceptable (!), median of 22 intubations required to reach this level. Paper open access here.
Ospina et al. in Rev Colomb Anestesiol, 2014: 764 ETIs performed by 4 anaesthesia trainees. Confusingly, they rate the level at which 75% of trainees reach 95% success (what does this mean in real life?) as a mean of 65 cases. Read the paper here and comment if you understand it better!
What does this quick search say to me? Firstly, there is a large discrepancy between some sources of the literature, but this is probably due to the dramatic heterogeneity of the study designs and outcomes. If you accept 90% success rate as acceptable for intubation proficiency (and, to be honest, I don’t), to be sure of your skills you need to make sure you put in at least 75 tubes. If your aim is “mastery” this figure is likely to be far higher…but then becomes an almost philosophical argument about the nature of mastery and the absence of any form of certainty in real life.
Herewith the presentation that Ross cobbled together for the candidates preparing for anaesthesia finals, to give an idea of the trends and new tools in airway management at the current time. Mostly pictures, but the lecture notes (with all the references) can be downloaded as a PDF here:
Some edits and new content on the go here at OpenAirway:
SASA Airway Guidelines (published December 2014 but only distributed in March 2015) added to the Algorithms page
Great visual cognitive aid on plans for the unanticipated difficult airway from NHS Lanarkshire (via the Scottish Airway Group) added to the Algorithms page
Folks are frequently reporting that our C-MAC Pocket Monitor is not switching on when they plug it in to a blade and want to use it, without realizing that it automatically goes into a hibernation mode if left in the open position for more than 15 minutes. Check out this quick AirwayHowTo video on solving this problem:
Presentation for the 19th World Congress of Disaster and Emergency Medicine (combined with EMSSA 2015) in Cape Town. Click on the fullscreen icon to see it in a more appropriate aspect ratio
Open access meducation for all aspects of airway management