Tim Leeuwenberg embarks on a near-thesis on the value of checklists, with special emphasis on airway management. An excellent read on the KI Doc blog:
AirwayHowTo: Leak test a flexible endoscope
Flexible fibreoptic and video endoscopes are fantastic but expensive pieces of equipment. In order to be maintained in top working condition, they need a little tender loving care. A particular problem occurs when the sheath of the scope becomes damaged or cracked, allowing fluid (especially corrosive cleaning solutions) to enter the inner workings of the scope, causing irreparable damage. The inner workings of the scope are a sealed environment. The patency of the seal – and thus the presence or absence of any damage – can easily be determined by performing a leak test. Although this is usually performed by medical technologists who are looking after the scopes, it can just as be performed quickly by the user while the scope is being prepared, or just before cleaning. Spend 100 seconds watching this brief, unadorned video which will walk you through the process. The demonstration here is using our Storz equipment, but is very similar regardless of the make or model of endoscope.
Combination of King Vision VL & AScope for Intrathoracic Goitre
@fibroanestesia comes up with some interesting ideas. Here they use a combination of the AScope3 (a disposable flexible video endoscope) and the King Vision video laryngoscope to perform a highly controlled intubation in a patient with an intrathoracic goitre. They have obviously pre-assessed this patient and concluded that the risk of failed intubation or positional loss of the intrathoracic airway due to compression is minimal.
Edible surgical airway model
What a great idea. Consume, rather than be consumed by your fears 😉 Credit to Rob Bryant and his team.
Cormack-Lehane Grading Examples
Here are some real-life examples of Cormack-Lehane classification of laryngoscopic view taken with a video laryngoscope. Although initially described for direct laryngoscopy in obstetric patients, it is a useful descriptive system in many settings, but is frequently misreported and/or misunderstood. We will continue to expand the set as we collect good images.
Original and revised (Yentis & Lee, 1998) CL grading:

Colour-coded to make it a little easier to read:

…and here from the CoPilot VL material, a more anatomically-correct sketch which shows the distinction between 2a and 2b clearly:

Cormack–Lehane 1:
Cormack-Lehane 2a:
Cormack-Lehane 2b:
Cormack-Lehane 3:
Cormack-Lehane 4:
See the original article by RS Cormack and J Lehane in Anaesthesia, 1994;(39):1105-1111.
Various modifications to this scheme have been proposed for use with video laryngoscopy (VL), including suggestions by Cook and Fremantle:


TotalTrack for Intubation in OSA
The TotalTrack is a new video laryngeal mask that allows intubation through the device without interruption of ventilation. Recruitment of the first independent clinical trial is well underway in Cape Town, with European studies nearing commencement. Here is an example video taken with the device, showing intubation in a patient with severe obstructive sleep apnoea (OSA).
Bougie-assisted intubation snagging on arytenoid
This common problem is worst with small bougies, such as in this paediatric example of a child with severe burns and a difficult airway. The bevel of the ETT allows the tip of the tube to stick out right (laterally) of the bougie and snag on the right arytenoid cartilage. This can be remedied by withdrawing the ETT slightly (to disengage it from the arytenoid), effecting a one-quarter counter-clockwise rotation of the ETT on the bougie (bringing the bevel and tip of the ETT into a superior midline position snug with the bougie), and then advancing again.
The Elaine Bromiley Case
Kudos to both Nicholas Chrimes and the Bromiley family for this excellent learning resource. Free lessons stemming from the bravery and compassion of others.
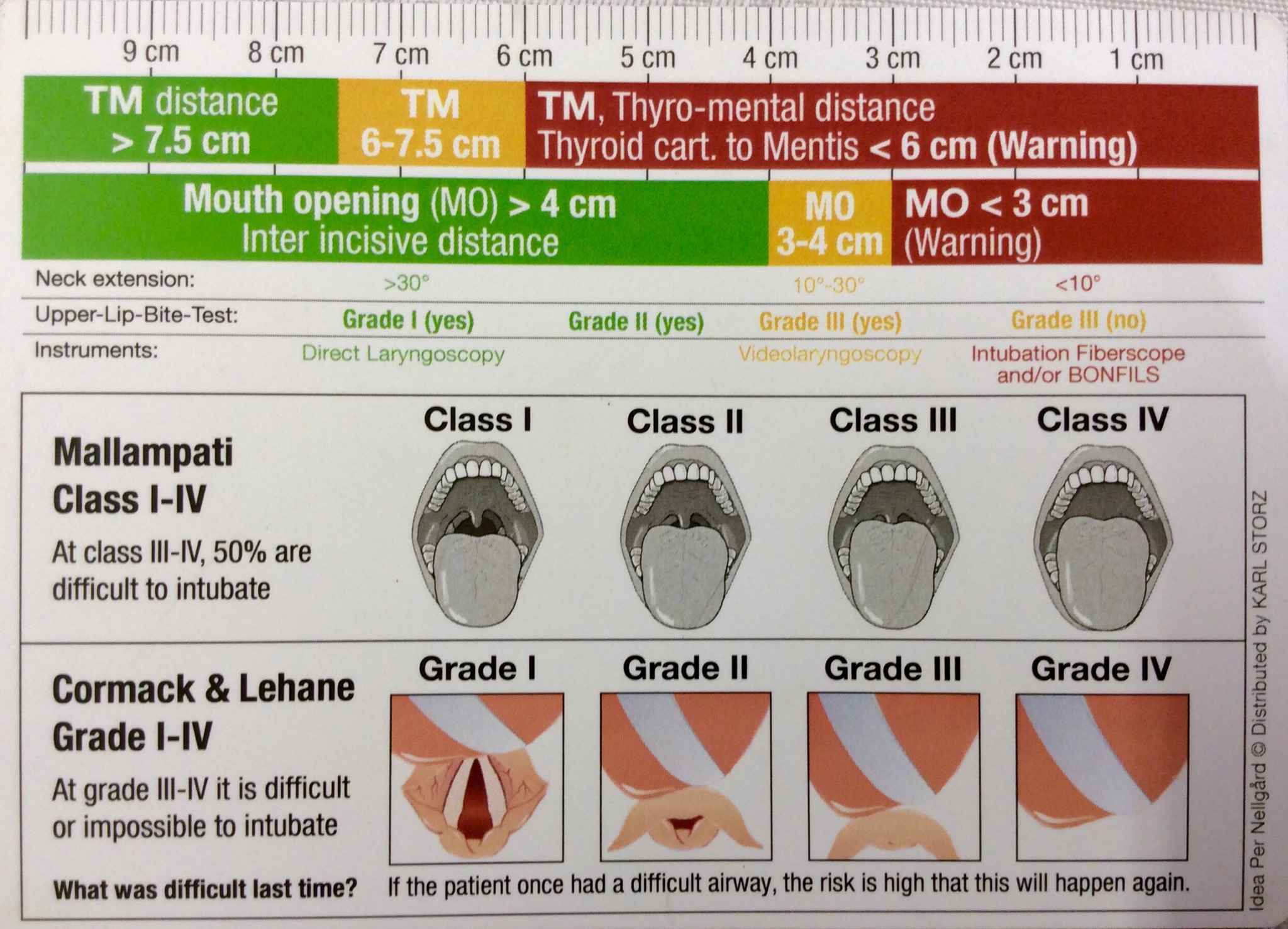
Airway Assessment Cue-Card
Picked this up at the Storz booth at a recent meeting. Printed on a 10cm piece of what looks like fairly hard-wearing plasticized card, it looks like it might survive in a pocket or bag for a fairly long time, and can be used to make direct measurements. Useful or gimmick? What do you think?
Supraglottic-guided intubation through 3gLM
Blinded intubation through the 3gLM SGA, as viewed by a video endoscope riding inside a Parker Flex-Tip ETT.
You must be logged in to post a comment.