OpenAirway has been collaborating with the UCT Department of Anaesthesia & Perioperative Medicine and the Southern African Society of Anaesthesiologists to include anaesthesia guidelines and reference materials in the Essential Medical Guidance (EMGuidance) app. Although only currently targeted at South African medics, this free app is accessible to all registered medical practitioners, and includes georeferenced guidelines from around the country. The content is continually being updated, with some exciting new developments just around the corner.
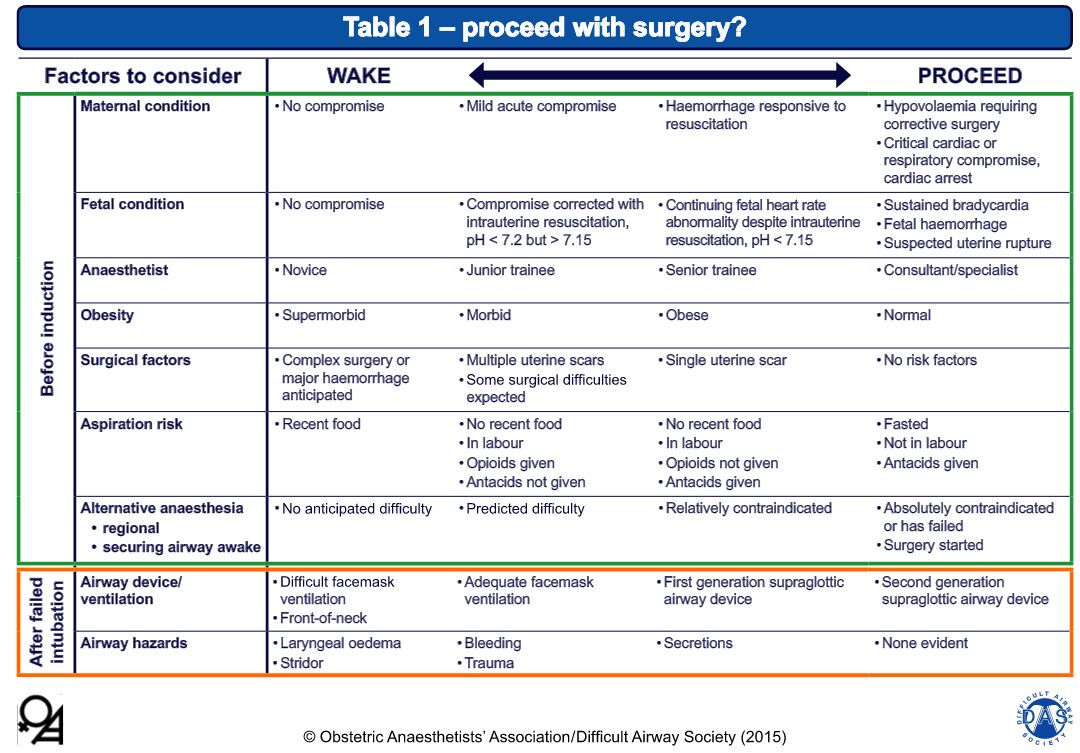
The guidelines are presented as a ‘Master Algorithm’ and several sub-algorithms to deal with specific aspects of obstetric airway management, and a guide to making the decision to awake the patient or continue with surgical delivery after an airway event:
Decision guide for awakening or proceeding with surgery, from the guidelines.
Some thoughts (COI – the author did provide feedback on the draft algorithms):
Stressing good positioning for airway management is absolutely critical in this population, and especially in practice environments where patients tend to have a high BMI (a common situation in our South African setting). The guidelines include ramping and the ear-to-sternal-notch (E2SN) position.
The inclusion of cricoid pressure will inevitably spark the usual debate, but it is this author’s contention that this is likely an appropriate use until more evidence to the contrary emerges. The guidance to consider CP reduction or release in the event of difficulty is apt.
The inclusion of gentle face-mask assisted ventilation during RSI is a welcome inclusion. Will we see NPO2 or HFNC included in later editions as more outcomes evidence emerges?
Advocating the use of VL in obstetrics certainly sounds like a good idea, but is not attainable for most of the developing world. This is a huge area for growth/research – the development of low-cost VL solutions.
This is a great step forward in promoting safe airway management and guiding training in a particularly dangerous corner of our practice.
For some more thoughts and images, here is a Prezi on the subject presented at the SASA Difficult Airway workshop in 2014:
Open access meducation for all aspects of airway management