Clinical video demonstrating a collection of techniques to facilitate elective intubation for a patient with an unstable cervical spinal injury in caliper traction. Note the sideways introduction of the VL blade due to limited space for the VL handle, optimisation of the view (‘Rule of 3’), use of a coude-tipped bougie (introducer), and the 3-part technique to advance the endotracheal tube when it catches on the arytenoid cartilage (pull tube back to disengage, rotate 90 degrees counterclockwise, advance tube).
Tag Archives: bougie
VLVids: Airtraq intubation using a bougie
Demonstration of an unhurried intubation using a bougie preloaded in the reinforced endotracheal tube in an Airtraq optical laryngoscope with Airtraq Cam video adapter. You can note ideal positioning of the Airtraq (“Rule of 3”) and the steering ability of a coude-tipped bougie.
VLVids: Room for Improvement!
This real-life videolaryngoscopy example (RSI of a patient with a head injury for craniectomy) shows some commom errors, and room for improvement. Three major areas that could be better to spot here:
- Less-than-ideal positioning of the VL blade. The tip is too deep (over the epiglottis, rather than in the vallecula), which reduces the available space to manipulate both VL and ETT, the field of vision, and the ability to perceive the approach of the ETT.
- Quick suctioning of the secretions/saliva/mucus would reduce the risk of losing the view or the patient aspirating.
- An introducer (stylet/bougie) would greatly assist passage of the ETT through the cords.
VLVids: Use an introducer!
A classic example of good videolaryngoscopy technique being thwarted by not always using an introducer (stylet or bougie). Note the clinician performing the intubation gets perfect, optimised VL view (Rule of 3), but then struggles to pass the ETT anteriorly enough, losing time. Although this was no problem for the well-oxygenated patient in this case (and the intubation is still under 45 seconds duration), in a critical case it can lead to desaturation, frustration, and possible intubation trauma.
Brimacombe technique
This came up recently during an M&M discussion of a very challenging spinal surgery/airway case. Here’s a quick overview of the technique:
Critique? These videos are all unscripted, so please comment so that we can improve them over time!
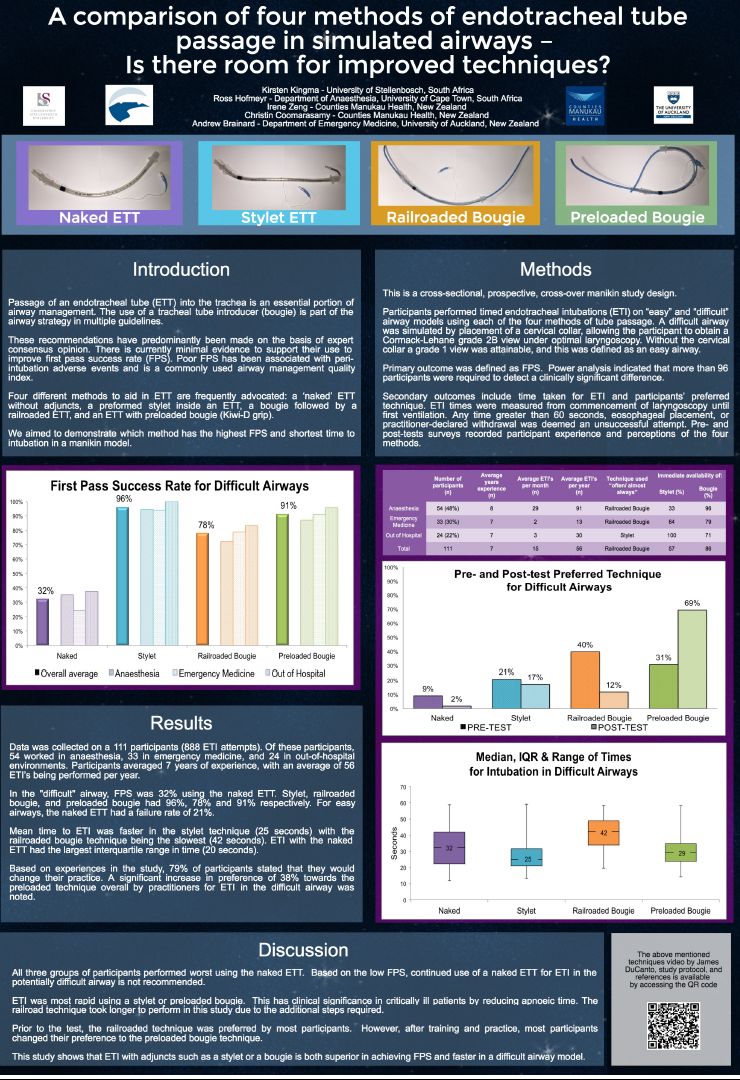
Four methods of endotracheal tube passage in simulated airways – Poster from ICEM 2016
Here’s the poster by Kingma, Hofmeyr, Zeng, Cooramasamy and Brainard that has generated a fair amount of interest (>10k impressions on Twitter). Full analysis hopefully coming soon to a journal near you. Bottom line? In a difficult airway, you’d best be using a bougie or stylet, no matter who you are. As far as bougies go, preloading rather than railroading is faster and seems better. Click on the image for a full-resolution PDF (2Mb).
Want to talk about this? Comment below or ping @surferkirst @rosshofmeyr @TheSharpEndCrew on Twitter!
Nice summary of helpful airway techniques
Great post on EMDocs covering useful airway techniques, which is helpfully referenced. Not really fair calling the concepts ‘novel’, as most have been around for some time, but are certainly not in ubiquitous use!
Click here for the post…and kudos to Joe Rodgers and EMDocs for the good work 🙂
Instructional Bougie Videos on HQMedEd
Kudos to Yen Chow (@TBayEDGuy) for alerting us to these two useful instructional clips on the HQMedEd page:
Time to get down and bougie?
Bougie-assisted intubation snagging on arytenoid
This common problem is worst with small bougies, such as in this paediatric example of a child with severe burns and a difficult airway. The bevel of the ETT allows the tip of the tube to stick out right (laterally) of the bougie and snag on the right arytenoid cartilage. This can be remedied by withdrawing the ETT slightly (to disengage it from the arytenoid), effecting a one-quarter counter-clockwise rotation of the ETT on the bougie (bringing the bevel and tip of the ETT into a superior midline position snug with the bougie), and then advancing again.
https://www.youtube.com/watch?v=DvnQL56FHZ8&feature=youtu.be