Over the past two weeks, I have been involved in three cases where all means of laryngoscopic intubation failed – including multiple different blades, introducers and highly skilled hands – and the airway could only be intubated with a flexible fibreoptic ‘scope. These three cases illustrate the type of pathology that can make even video laryngoscopy (VL) difficult or impossible:
A morbidly obese patient in traction with a high spinal injury
A patient presenting with late-stage, advanced laryngeal carcinoma with both supra- and infraglottic involvement and masses
A child with Pierre-Robin Sequence presenting for mandibular distraction surgery.
The well-known thoracic anaesthesia guru, Prof Jay Brodsky, has written a succinct and simple overview of the use of fibreoptic bronchoscopy (FOB) in thoracic anaestheisa, which is equally applicable to the modern flexible video endoscopes. If you are looking for a brief primer (including the appropriate use for placement of bronchial blockers and double-lumen ETTs), read the article on the Airway E-Learning site here.
Importantly, he elucidates the reasons for becoming proficient in the clinical placement and confirmation of DLTs without the use of a FOB, which is of particular relevance here in the developing world.
A quick video aimed at introducing our clinicians to a new piece of equipment, but potentially a useful overview of this type of device to anyone who may make use of portable flexible ‘scopes.
…to come and have great fun on our courses at UCT. This from the hands-on airway endoscopy afternoon run recently for the Department of Anaesthesia’s own staff:
Despite making a previous post and video to explain the way to make sure the device switches on, I regularly get told that the Pocket Monitor (PM) for our C-MAC video laryngoscope is not working/charging/switching on. This is in fact a design feature to prevent accidental activation or discharge. Watch here to find out more:
Thanks to the lovely Sam Adams for playing along…good career in acting if anaesthesia were to ever become boring!
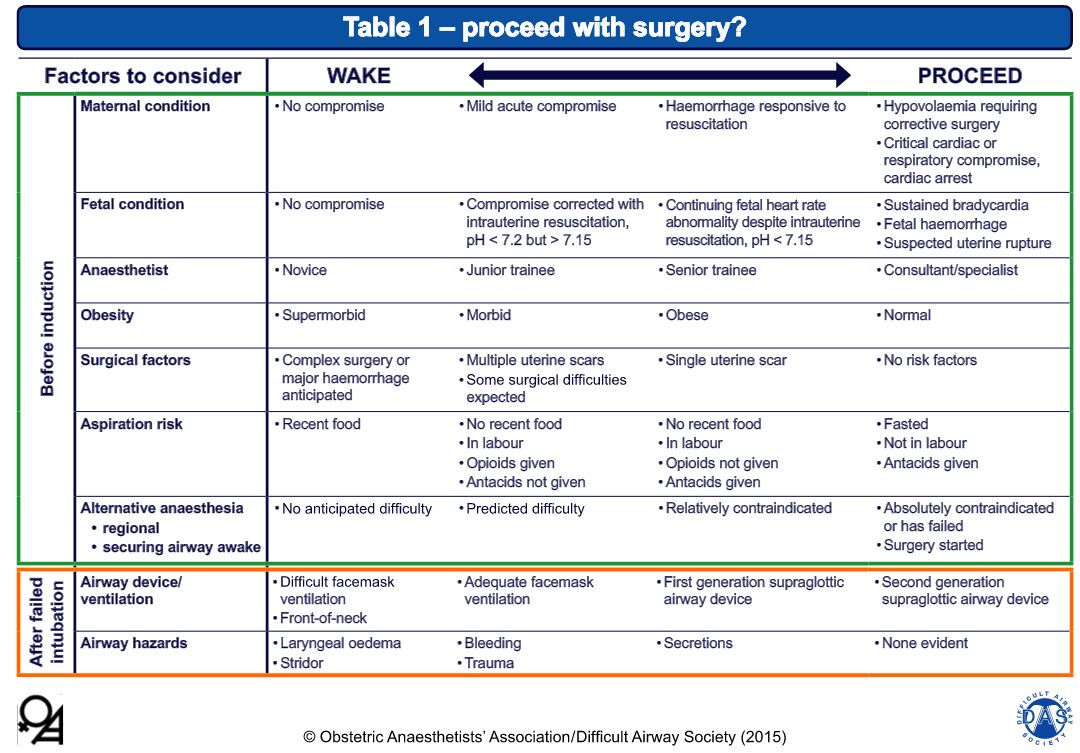
The guidelines are presented as a ‘Master Algorithm’ and several sub-algorithms to deal with specific aspects of obstetric airway management, and a guide to making the decision to awake the patient or continue with surgical delivery after an airway event:
Decision guide for awakening or proceeding with surgery, from the guidelines.
Some thoughts (COI – the author did provide feedback on the draft algorithms):
Stressing good positioning for airway management is absolutely critical in this population, and especially in practice environments where patients tend to have a high BMI (a common situation in our South African setting). The guidelines include ramping and the ear-to-sternal-notch (E2SN) position.
The inclusion of cricoid pressure will inevitably spark the usual debate, but it is this author’s contention that this is likely an appropriate use until more evidence to the contrary emerges. The guidance to consider CP reduction or release in the event of difficulty is apt.
The inclusion of gentle face-mask assisted ventilation during RSI is a welcome inclusion. Will we see NPO2 or HFNC included in later editions as more outcomes evidence emerges?
Advocating the use of VL in obstetrics certainly sounds like a good idea, but is not attainable for most of the developing world. This is a huge area for growth/research – the development of low-cost VL solutions.
This is a great step forward in promoting safe airway management and guiding training in a particularly dangerous corner of our practice.
For some more thoughts and images, here is a Prezi on the subject presented at the SASA Difficult Airway workshop in 2014:
The newest edition of the Anaesthesia Tutorial of the Week (ATOTW #321) covers the much underestimated but critically important topic of predicting and managing difficulty in face mask ventilation. Irish anaesthetists Jonathan Holland and Will Donaldson have created a useful resource for anyone studying or performing airway management, or refreshing for exam purposes.
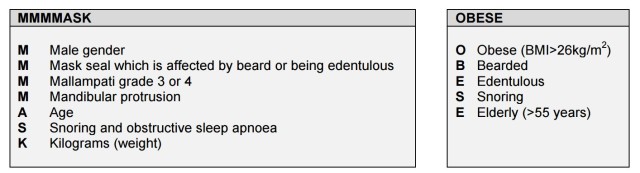
The authors discuss the predictors of difficult mask ventilation and report/propose another two mnemonics, to add to the existing stable (MOANS, BONES, etc):
Two mnemonics for prediction of difficult face mask ventilation. Source: ATOTW 321
I’ve always used MOANS for mask factors (like I use LEMON for laryngoscopy), but all these mnemonics cover the same ground. MOANS, for instance, stands for
M Mask seal factors, like beards, NGTs, odd shaped faces
O Obesity and causes of Obstruction, like tumours/angioedema
A Age extremes (the elderly and very young)
N No teeth (or nasty dentition)
S Snoring and Stiff lungs (the latter being issues like inhalation burns and acute bronchospasm, where the higher pressures required increase the risk of gastric insufflation and Splinting of the diaphragm)
As you can see, they are all much the same, although there are a few things that are not covered by every algorithm. The purist would point out that obesity is defined as a BMI of >30 kg/m2, not 26 as stated in the table.
Hollan & Donaldson’s flowchart for management of difficult face mask ventilation. Source: ATOTW 321
The authors then present a useful flowchart for addressing unexpected difficulty, which is quite sensible. It is much in line with the DAS guidelines and other algorithms for general airway difficulty, and useful for instruction. Of course, in a dire emergency, using a cognitive aid such as the Vortex would be effective.
Open access meducation for all aspects of airway management