This year’s International Airway Management Meeting was fully online, thanks for COVID, but SARS-CoV-2 certainly gave us lots to talk about. The meeting, held over 21-22 May, brought together 44 international experts for online presentations and very robust discussions, and had nearly 50 000 views online. The good news (if you missed it) is that the content is still fully available as an online recording (over 10 hours worth!), which you can access here:
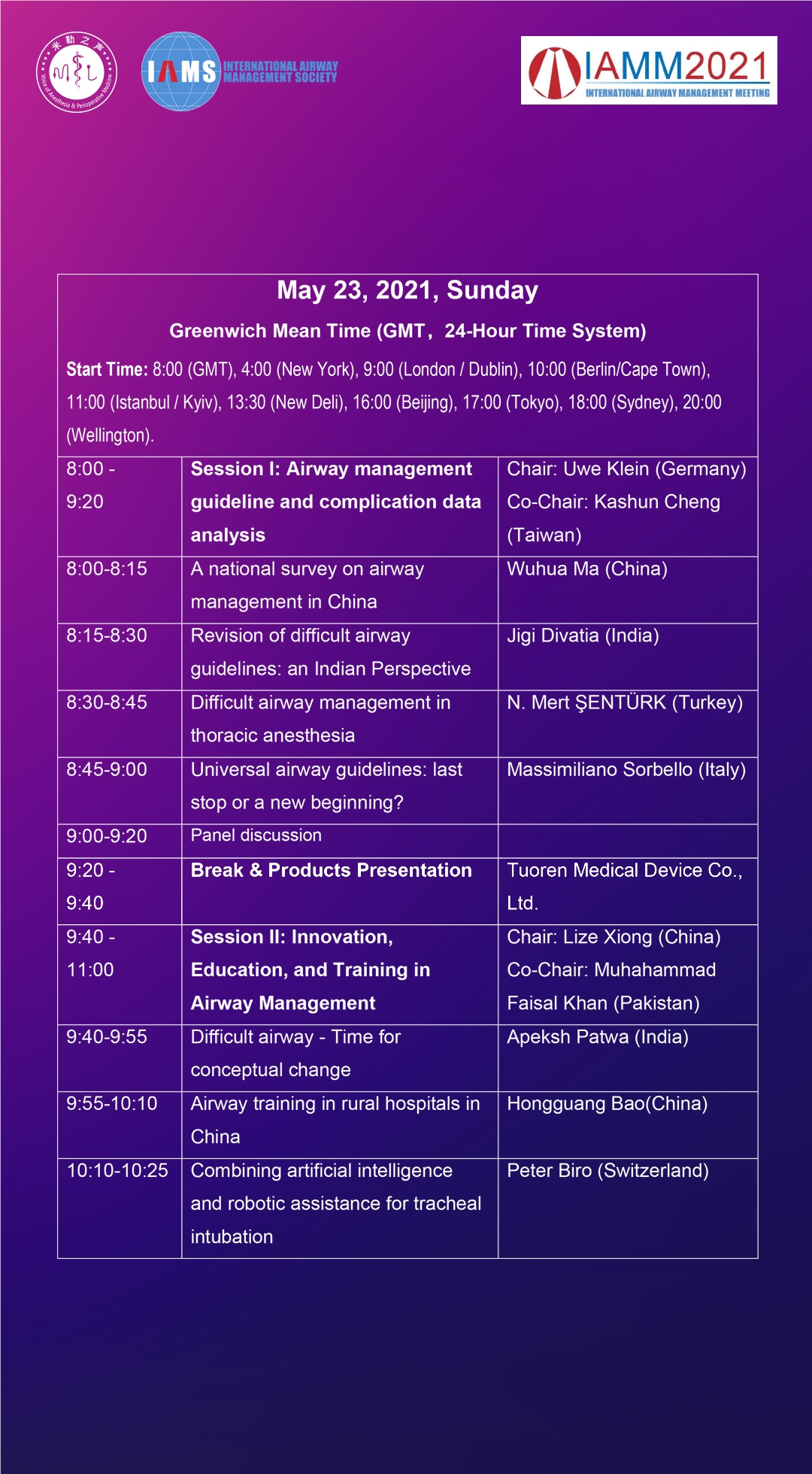
The full program is below. You can watch the recording on my talk on “COVID Airway Management: Principles, Projects, Pet Ideas and Proper Evidence” below or by following this link.
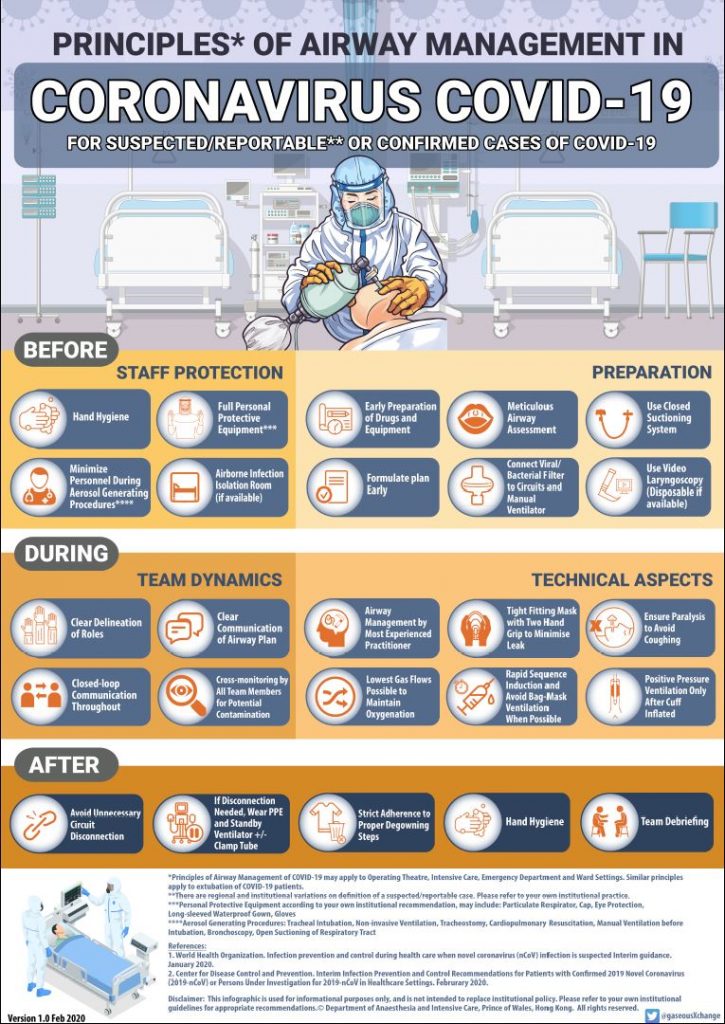
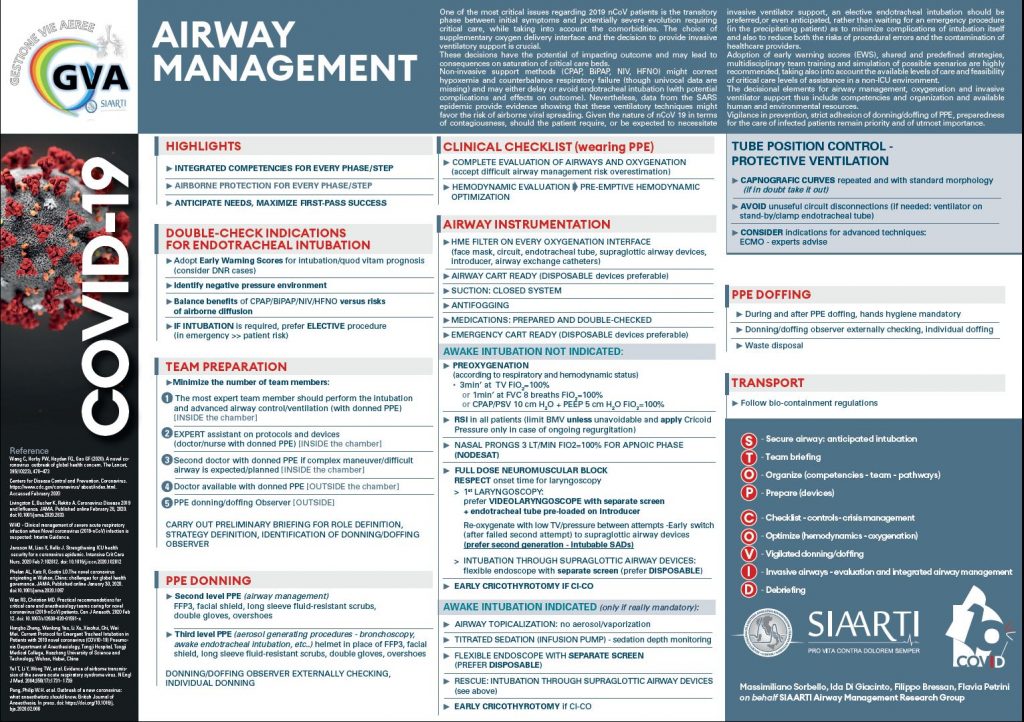
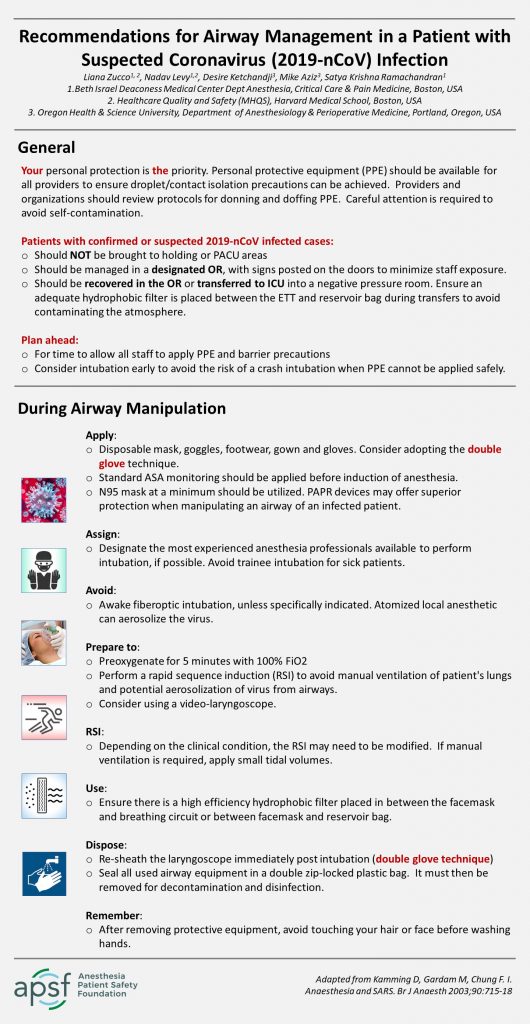
Yip, it’s on all of our minds right now. Want a one-stop shop for airway management (and other anaesthesia) resources for COVID-19? It’s here on OpenAirway: OpenAirway.org/covid-19-airway
A couple of examples of great work coming from the webs:
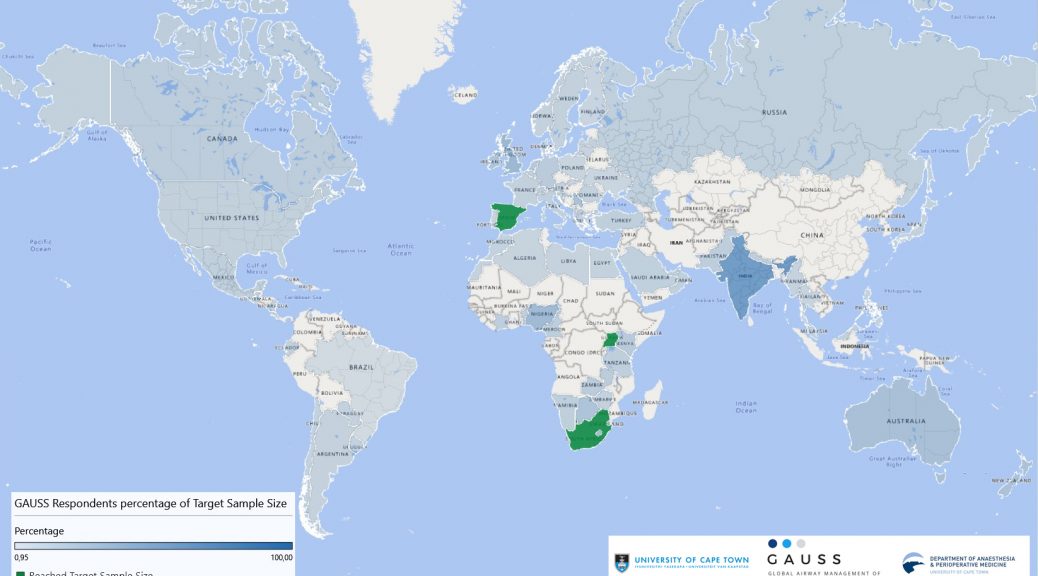
Have you shared your preferences, practice and experience with managing the airway in patients with unstable cervical spine injuries? We have representation from around the world but would still like to expand our sample! If your country is not dark blue or green in the map above, please add your voice:
New content – we’ve added a static page to OpenAirway to build up a resource of #FOAM content on airway ultrasound. There is quite a lot out there on the great big interwebs, but this should form a kernel of good stuff to get you up to speed, or learn a few nuggets. Please comment on the page if you have additional sources or ideas to suggest. You can find the Airway Ultrasound page here.
In the process of collating material for the Airway Ultrasound resources here on OpenAirway, the great free e-learning courses on usabcd have come to light. After registering with the service, you can access the following freecourses (and even take the tests, generating a course certificate):
You’ll need to register, add the courses to your cart and then check out (total fee 0.00) to gain access to the material. There are plenty of other modules, including FATE, FAST, lung ultrasound and TEE which can be accessed for a fee. Check it out!
Here’s a brief clinical example of dual endoscopy using the CMAC VL and VS (video stylet). This case was performed for teaching purposes, rather than a difficult airway. Note the endoscopic view appearing as a picture-in-picture is from the editing; the images are on two separate displays. (It starts a little late due to the author forgetting to press the record button on the device).
“Dual endoscopy” refers to using two devices – usually a video laryngoscope and a rigid or flexible endoscope – to manage an airway. The Bonfils (or Shikani or Levitan) optical stylet is often used in this context. Performing dual endoscopy provides “three levels of protection”:
If the glottic opening is easily seen with the laryngoscope, the rigid endoscope simply acts as an ideally shaped or steerable stylet to introduce the tube
If the view is poor (CL grade 3 or 4), the laryngoscope can be used to guide the tip of the ETT and endoscope “into the ballpark”, and then the final positioning of the tip of the tube through the vocal cords is achieved with the endoscope.
If the airway is badly soiled or swollen (eg. ongoing bleeding or angioedema), the endoscope can be used as a lightwand for a transillumination technique. (Remember lightwands, anyone?)
Here’s a brief informal video explaining the first two points, using the CMAC VL/VS:
Another dual endoscopy approach is “VAFI” (video-assisted flexible/fibreoptic intubation), where a VL is used to help place a flexible endoscope, whereafter the rest of the intubation is continued using the flexible. Several good case reports of this technique are described in the literature.
Here’s a brief clinical example of dual endoscopy using the CMAC VL and VS (video stylet). This case was performed for teaching purposes, rather than a difficult airway. Note the endoscopic view appearing as a picture-in-picture is from the editing; the images are on two separate displays. (It starts a little late due to the author forgetting to press the record button on the device).
Some of the newest devices (eg. CMAC 8404; Glidescope Core monitors) allow both images to be displayed on the screen simultaneously, either as a “picture in picture” view, or side by side. If using the latter, orientating the images so that the VL is on the left and endoscope on the right is convenient, as this matches the two hands being used. Here’s an example, again in a patient with an easy airway, but simulating CL3 view:
Dual endoscopy using CMAC3 and Bonfils. It would have been good to have warmed the Bonfils before starting, to prevent the fogging of the distal lens.
Herewith my 10-minute “Meet the Expert” presentation for the 2018 Euroanaesthesia congress. Click on the image to access. Selected references available in the zip file below.